If your passwords are less than 8 characters long, you must change them immediately, according to a recent study from Hive Systems.
Your online security is important and this study demonstrates how long it would likely take the average hacker to crack the passwords safeguarding your most important online accounts.
Short and simple passwords can be cracked in a matter of seconds. Long and complicated ones? Trillions of years.
The below question and answer were published in the New Zealand Aged Care Association industry ‘In-Touch’ newsletter (19th February 2016).
Question:A member asks “if we purchase a comprehensive quality management system from a provider how assured are we that the system will meet full compliance, come certification and surveillance audit time, as requirements and compliance expectations change frequently?
NZACA Clinical Advisor Answer: “You should be purchasing a complete quality management system that will comply with the Health and Disability Standards specifications, health and safety requirements and meet DHB/ARRC contractual requirements.
The provider of the system would normally initially tailor the full quality management package to reflect accurately the site specifications, H.R. component, and best practice guidelines, after consultation with the owner and management on site. These documents need to be site specific. The provider will normally contract to the site, which sets out obligations between the provider and the site management.
The contract will include the full review and updates of policies and procedures on a bi-annual basis, unless specified more frequently, to keep documents accurate and reflective of best practice. There may be an educational element provided within the contract as well, to benefit staff knowledge and skills. There is normally a good document control system in place and cross referencing of information where required.
Quality management systems are reliant on the skills and knowledge of the site personnel working with them, the way the system is managed and the outcomes/reviews, content and information extricated from the use of the system to improve quality care provision/outputs. The documentation system is reflective of the people using them, and the depth to which documentation and information is created, analysed and utilised for improvements.
Auditors on site rely on the provision of robust up-to-date policies and site adherence to them. Partial attainments can sometimes result from staff deviating from, or not following, their sites actual policies or processes as outlined in their quality management system.”
Where can you get such a system?
Here at Healthcare Compliance Solutions Ltd we provide the services described above and noted as being optimal for achieving excellence in care and audit outcomes. To see a brief video about the Aged Care software update and now in use by over 3,800 users in NZ, click here.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2020-03-17 16:37:002024-09-24 07:18:00Quality Management Systems
Clinical documentation and clinical management relate to section 1.3.1 to 1.3.8 of the Health and Disability Services Standards and are referred to in section D5.4 of the ARRC. There are key reference documents which provide reference at residential care facility level which should be used in conjunction and addition to your organisation policies and procedures. These reference documents include:
Age Related Residential Care (ARRC) contract
NZS 8134:2008 Health and Disability Services Standards
Clinical best practice (EBP) guidelines – eg; Lippincott
The Code of Health & Disability Consumers Services Rights 1996
Clinical documentation errors of any type noted during audits will result in partial attainments at best. This is an indication there could be risk associated with gaps in service. In a previous article about medication management we noted that even a single signature missing off an administration signing sheet was enough for the auditor to assign a partial attainment finding.
Below are some of thecommon compliance gaps which relate to clinical documentation:
General compliancegaps
Missed signatures off notations.Not dated.Not signed by the author with a full signature.No designation written with signature.Not legible.Inconsistent structure of resident files.Unclear or unsecured archiving of documents.Privacy breaches due to clinical documents placed in a situation that allowed unauthorized viewing.
Initial assessmentsincluding InterRai
Not completed within time-frames defined in ARRC.Baseline recordings at time of admission not recorded.Assessment outcomes not used as a basis of care planning to link assessment to goals and interventions.Additional detailed assessments not reviewed in a timely manner eg; six monthly to coincide with InterRai reassessments.Failure to re-assess for each period of admission eg; respite care.
Clinical risk
Assessment not describing risk.Risk not reflected in care plan interventions.Lack of risk reviews.Level of risk noted in interRai assessments not included in care planning
Progress notes
Not recorded in on a shift by shift basis.Lack evidence of regular registered nurse input.Writing beyond the bottom line of the page.Failure to put resident identifiers on each side of each page (this applies to other clinical documents as well).Lack evidence of interventions being implemented.Lack evidence of RN response to clinical symptoms reported by care staff.Lack of evidence of rationale for PRN medication administration or the resulting effect.
Short TermCare Plans
Not developed for changes in clinical status eg; increased pain; infection; wounds, change in medication (to allow evaluation of effectiveness).24 hours plans not developed for residents displaying behaviours of concern (challenging behaviours).Not evaluated regularly (I suggested at least once every 7 days) by a Registered Nurse.Not recorded as resolved or transferred to Long Term Care Plan.Not developed to implement instructions included in General Pracitioner consultation plans recorded in notes.
Long TermCare Plan (LTCP)
Not reflective of all presenting potential and actual medical / clinical problems.Not documented within 3 weeks of the date of admission (ARRC requirement).Not changed at the time of health status / functional change.Interventions not reflective of each medical diagnosis.Interventions not changed within LTCP to reflect changes recorded in care plan evaluations.Frequency of clinical assessment for each actual clinical presentation eg; pain.Do not clearly indicate the level of function, assistance required for each component of care / support.Do not clearly evidence input and instruction from Medical or Nurse practitioner / Physiotherapist, Diversional Therapist, Dietitian,Psychiatric services for the elderly etc.
Care PlanEvaluations
Review of care plans not reflecting changes in residents health status as they occur.Not reflective of how well the care plan goals/ objectives have been met since the previous evaluation.Not completed within ARRC defined time-frames (at least six monthly).
Multi-DisciplinaryInput
Lack evidence of MDT input into care plan reviews and/or evaluations.Lack evidence of resident, Next of Kin (NOK) / Family / Whanau / EPOA input into assessment and care planning.Lack of evidence of timely referral in response to clinical presentation eg; unintentional weight loss not referred to Dietitian.Failure to evidence implementing instructions ofMedical or Nurse Practitioner eg; B/P to be recorded daily for the next 7/7 may be noted in the medical consultation notes however not evidenced as having been done.Lack evidence of notification to NOK / EPOA relating to resident adverse events, change in health status, medical consults etc.
Policy andprocedures
Not consistent with service delivery as noted in clinical documentation.
Internal audits are available through the online HCSL quality system utilised by our clients which allows tracking of compliance status and corrective actions as part of on-site quality and risk management. This means when the auditors arrive, there will be no surprises and you’ll know you’ve achieved excellence in care in conjunction with providing a compliant service.
If you have any comments to make about this article, please contact us here.
When undertaking a change management process in care facilities, I’ve identified 5 distinct phases of reaction from managers and staff. These have often occurred after I’ve been appointed to perform the role of statutory (temporary) manager by a DHB. This is generally after risk to residents has been identified following an audit or a serious complaint.
As a temporary manager, often there is a facility manager in place however for a range of reasons doesn’t have the resources or knowledge to meet the needs of the residents to a standard that satisfies audit outcomes.
Phase 1 is on first arriving and there is relief on the part of the staff and manager (if there is one) on the basis they have the view that I’m there to ‘save the day’, make things right and then they can get on with running things. Comments such as “you should have been called in a long time ago” are common.
Phase 2 is where the staff and in place management start to realise that I’m not going to do all the work for them and my role is that of mentor and coach. Further to that the role includes assistance with obtaining necessary resources to support clinical and operational practices. This is where push-back and resistance starts to show as people resist change and try to hold stead-fast to those practices that have got them to the point they’re at. As pressure increases for change to occur, resistance increases and at times sabotage of the new way of doing things starts to appear. As one provider put it recently “they’re ever so nice to your face and will stab you in the back”. The denial phase plays out and the anger phase starts.
Phase 3 is a time when divisions start between those who want to embrace change knowing it’s intended to improve and make the workplace safer for staff and more so, safer for residents; and those who don’t have insight to recognise the need for change. The need for people to remain in their comfort circle doing what’s known and predictable is incredibly strong for a large number of people. This slows momentum and the temporary manager starts to get the blame for things being wrong. Such comments as ‘it was all fine before the DHB stepped in, they just need to back off and let us get on with it’ are also commonplace in this phase. Sometimes senior staff at the facility will contact their DHB and say the temporary manager is unreasonable, not doing anything and needs to be removed. All as an attempt to get rid of the person they see as pushing them outside their comfort circle and affecting maintaining of the status quot. The bargaining phase can continue for quite some time but this often depends on how direct and steadfast the response is to the bargaining strategies.
Phase 4 occurs when there is the start of the depression phase and realising that solid work, participation by all and a willingness to take on new ideas and learn new ways of doing things needs to occur. The real work has started by the willing few in the early phase and continues and now the collective change can start to be evident.
Phase 5 is acceptance that the temporary management or change management process was necessary. Staff start to commend the new way and embrace new ideas recognising that things are actually better now than they’ve been before. As people always have choice about coming on board with change or leaving, invariably there are some staff and sometimes managers or even members of Governance who continue to resist seeing a new way is needed and those few will leave the organisation or continue to resist.
I’m able to observe which phase an organisation is operating in by the response of those working there and was intrigued to read of exactly this same set of steps in a book titled ‘Expert Secrets’ written by Russell Brunson. Some of you who are familiar with the work of Elisabeth Kübler-Ross will also recognise these phases as reflecting her stages of grief.
Acceptance is hard as people take the need for change as a criticism when in my view, people don’t fail; systems do!!
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-11-15 10:46:002024-09-24 10:08:28Understanding the Change Process
All mobile device compatible so you can be with your residents rather than stuck in the office!
HCSL bringing cost effective, specifically designed tools for the New Zealand residential care sector. The Corporates have their tools, why shouldn’t you have the same advantage?!
To find out more and get a no obligation free quote for use contact us here.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-11-12 14:49:002024-09-24 10:10:46Clinical online tools for Aged Residential Care
Mobile app now available for conducting your residential care ARRC specific internal audits.
There are a full range of internal audits pre-loaded ready for use. Collectively, these audits reflect the criteria Certification auditors will be checking.
This process gives you the opportunity to be sure you’re on track with achieving compliance. The findings auto-populate into corrective action tables which prompt timely addressing of these corrective actions. This system syncs with your main computer system and makes reporting to management and Governance boards very easy.
The Certification auditors (after given specific access authority with your permission) are also able to access the results of the internal audits you’ve completed.
To view a brief video on the use of this system, click here.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-17 09:43:002024-09-24 10:18:40HCSL Mobile app for Internal Audits
Topics included: Quality & Risk Management, Clinical Leadership, Clinical Documentation, EPoA, ARRC, Communication and Difficult Conversations
I am writing this endorsement on behalf of my colleague and myself, in relation to our attendance at the study day you hosted 5 July 2017.
The topics you presented were most relevant to our Registered Nurse role within the aged care sector, and between us both provided new learning opportunities, as well as refreshing the current knowledge we already held.
You addressed each session in a professional and engaging manner that held our attention, complemented by comprehensive written material as well as PowerPoint presentations, along with plenty of opportunity for questions and comments from the floor.
Gillian you are one of very few speakers that is able to hold my attention for more than one session let alone a whole study day, a perfect balance between speech and conversational styles!
We were also most impressed by the quality of the complementary gift bag that was given to each attendee containing not only goodies to help us through the day, but with something to take back to the workplace, I acknowledge both Cubro and Ebos for their support with this.
The venue was great with easy access and good parking, and it was clean and refreshing providing plenty of comfort and personal space for those attending. I will be recommending my associates to make a note in their diary for next time. Thank you Gillian
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-08 16:26:002024-09-24 10:23:07Attendee Testimonial for Aged Care Education Study Day – July 2017
Dysphagia diets and a lack of understanding of how to implement them consistently, is increasing risk to residents in aged residential care services.
Texture modified diets are commonly used in aged care facilities to manage the risk of aspiration pneumonia and choking with eating and drinking. Residents with dysphagia may be placed on a texture modified diet following assessment with a speech and language therapist. However there are often a range of terms used for texture modified diets, and differing opinions on exactly how the diets should be prepared.
Confusion with terms, and the types of foods and fluids offered leads to increased risk of harm for the resident. This is particularly obvious when transferring from one facility to another. Information on texture modified diets is passed to the new facility who may use different terms. For example a site may report ‘this resident requires a soft diet’ and the interpretation of this diet at the new facility is to puree all food.
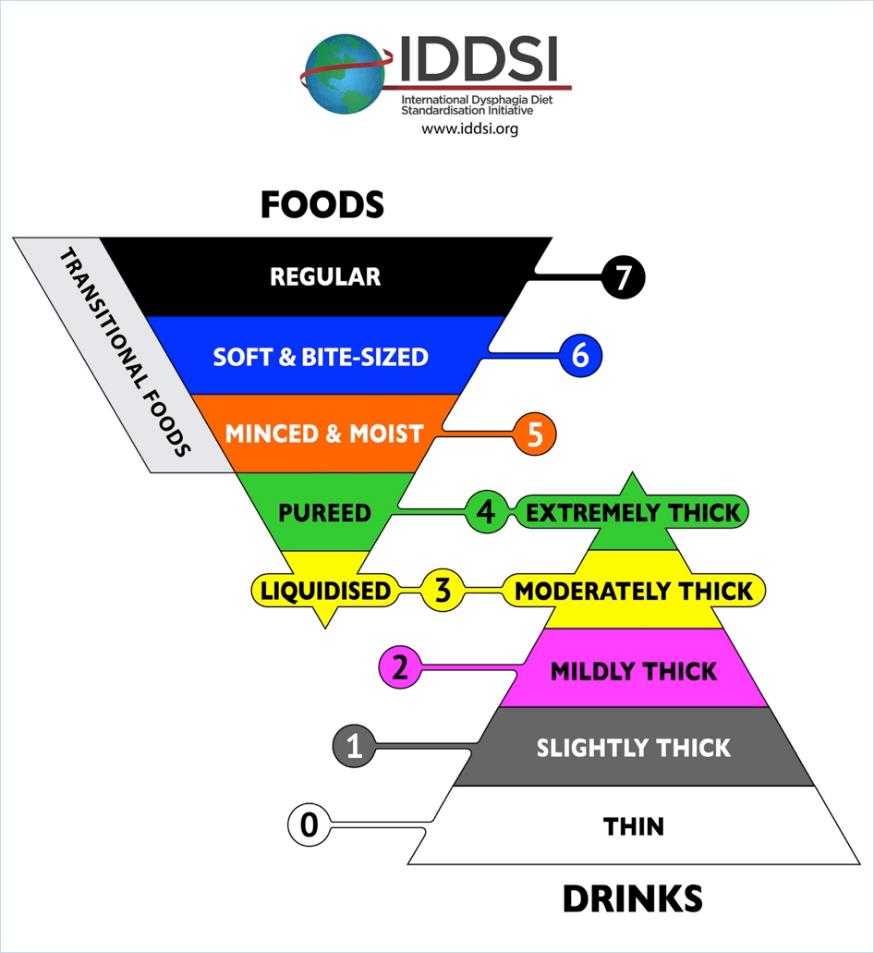
The International Dysphagia Diet Standardisation Initiative (IDDSI) is a framework to standardise terminology and offer simple testing methods to check that the preparation of the diets are correct. Dietitians New Zealand and Speech Language Therapists of New Zealand have endorsed in principle the IDDSI framework.
The goal is to reduce the risk of harm for our patients and residents due to miscommunication and poorly prepared texture modified diets. It is important to note that the framework relates to dysphagia diets only. Residents may be on a modified diet due to other factors not related to dysphagia. For example a resident with no teeth may need softer foods but can actually manage sandwiches.
The good news is that for many sites, there is very little change needed as they are already using the correct terms. The diagram above shows the new terminology and the minimal change in wording;
‘Smooth puree’ becomes pureed (which is also extremely thick fluids)
‘Minced and moist’ remains unchanged
‘Soft diet’ becomes ‘soft & bite sized’
Moderately thick and mildly thick remain unchanged for thickened fluids
The IDDSI framework assigns standard colours and numbers to assist with easily identifying texture modified foods and fluids. Some manufactures of texture modified foods and fluids are looking at ways to incorporate the terms, colours and numbers onto their food packaging.
Food and Fluid Preparation and Testing
The IDDSI framework offers simple tests to check that the thickness of the fluids or the size of the particles for modified foods are correct. The tests use forks, spoons, fingers or syringes – equipment that is readily available at sites.
With training and education on how to do these tests, kitchen staff and managers will be able to easily check their texture modified diets and thickened fluids are prepared correctly.
IDDSI App and Website
The IDDSI framework have developed many resources and videos to assist with the standardisation process.
or ask your dietitian and speech language therapist for more information.
Where to From Here?
Here are some small steps to help implement the IDDSI framework at your site:
Stop using any terms that are not on the framework. The term ‘mouli’ is not recognised and should not be used to describe a texture modified diet.
Download the app or look at the IDDSI website to familiarise yourself with the framework.
Try testing one of the textures you currently prepare. Does the ‘puree diet’ your site produce pass the spoon tilt test? Does the size of the minced food for ‘minced & moist diets’ fit between the prongs of a fork? Is the size of meat offered for residents on the ‘soft & bite size diet’ the size of your thumb nail?
Ask your dietitian or SLT for further training on the correct testing and preparation of dysphagia diets.
This article was contributed by Liz Beaglehole NZRD (Canterbury Dietitians) and Anna Miles PhD, Speech-language Therapist, Senior Lecturer, Speech Science, School of Psychology. The University of Auckland.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-07 11:57:002024-09-24 10:25:50Dysphagia Diets – Are we all understanding each other?
I have found that having Gillian’s (the HCSL) system available has been a huge help to our village. Documents are easily accessible at my fingertips and it hasn’t taken long to memorise some of the codes for the more frequently used ones.
If we are having trouble finding a document or we want to make any adjustments, Gillian is always very accommodating and helpful. She is easily contacted by telephone or email and if she is busy, always gets back to me as soon as she is able to. I particularly like that if I want to type into a document, Gillian makes this available.
When the documents are due for updating, Gillian takes care of this, printing all of the documents and putting them into new folders for us. She even delivers them personally, which is always a pleasure. I find Gillian very approachable and extremely knowledgeable and happy to share her knowledge.
Gillian assists us with our training requirements by coming to Chatswood and going through the annual compulsory subjects with myself and my staff. She is great at presenting and the passion about her work shows in the way she shares her own experiences with us.
I look forward to our continued working relationship.
Is a slip off a chair or off the side of the bed onto the floor a fall? Is a ‘controlled lowering’ by a staff member of a resident to the floor a fall?
When recording adverse events such as falls, it’s important for the purposes of consistent reporting and bench-marking that the same definition is used to define a ‘fall’. We suggest using the definition provided by the World Health Organisation (WHO) which states “A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level.” The WHO falls prevention guidelines also report that “Globally, falls are a major public health problem. An estimated 424 000 fatal falls occur each year, making it the second leading cause of unintentional injury death, after road traffic injuries.”
Working in aged care related services means you are interacting on a daily basis with those in the high risk category for falls. WHO also report for example, in the United States of America, 20–30% of older people who fall suffer moderate to severe injuries such as bruises, hip fractures, or head traumas. The Health Quality and Safety Commission New Zealand report “for every fall in hospital, there are five in aged residential care and another 40 at home and in the community. Between 2010 and 2012, a total of 200 people fell while in hospital care and broke their hips.“
The HCSL QA online bench-marking includes tracking of falls and falls related injuries so educating your staff to become familiar with the definition is important in ensuring data collected is accurate. Accurate data measurements also allow you to be aware of your start point for quality improvement projects which can then be measured at the end of a project to measure the degree of improvement.
In answer to the questions posed at the start of this article, if we apply the WHO definition, then both should be classified as falls. For those of you using the HCSL policy and procedure system, refer to the Falls Prevention Programme (document CS19) for more information on falls prevention.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2016-05-11 16:44:002024-09-25 02:42:14Falls – When is a fall not a fall?





{kind=link}