Topics included: Quality & Risk Management, Clinical Leadership, Clinical Documentation, EPoA, ARRC, Communication and Difficult Conversations
I am writing this endorsement on behalf of my colleague and myself, in relation to our attendance at the study day you hosted 5 July 2017.
The topics you presented were most relevant to our Registered Nurse role within the aged care sector, and between us both provided new learning opportunities, as well as refreshing the current knowledge we already held.
You addressed each session in a professional and engaging manner that held our attention, complemented by comprehensive written material as well as PowerPoint presentations, along with plenty of opportunity for questions and comments from the floor.
Gillian you are one of very few speakers that is able to hold my attention for more than one session let alone a whole study day, a perfect balance between speech and conversational styles!
We were also most impressed by the quality of the complementary gift bag that was given to each attendee containing not only goodies to help us through the day, but with something to take back to the workplace, I acknowledge both Cubro and Ebos for their support with this.
The venue was great with easy access and good parking, and it was clean and refreshing providing plenty of comfort and personal space for those attending. I will be recommending my associates to make a note in their diary for next time. Thank you Gillian
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-08 16:26:002024-09-24 10:23:07Attendee Testimonial for Aged Care Education Study Day – July 2017
Dysphagia diets and a lack of understanding of how to implement them consistently, is increasing risk to residents in aged residential care services.
Texture modified diets are commonly used in aged care facilities to manage the risk of aspiration pneumonia and choking with eating and drinking. Residents with dysphagia may be placed on a texture modified diet following assessment with a speech and language therapist. However there are often a range of terms used for texture modified diets, and differing opinions on exactly how the diets should be prepared.
Confusion with terms, and the types of foods and fluids offered leads to increased risk of harm for the resident. This is particularly obvious when transferring from one facility to another. Information on texture modified diets is passed to the new facility who may use different terms. For example a site may report ‘this resident requires a soft diet’ and the interpretation of this diet at the new facility is to puree all food.
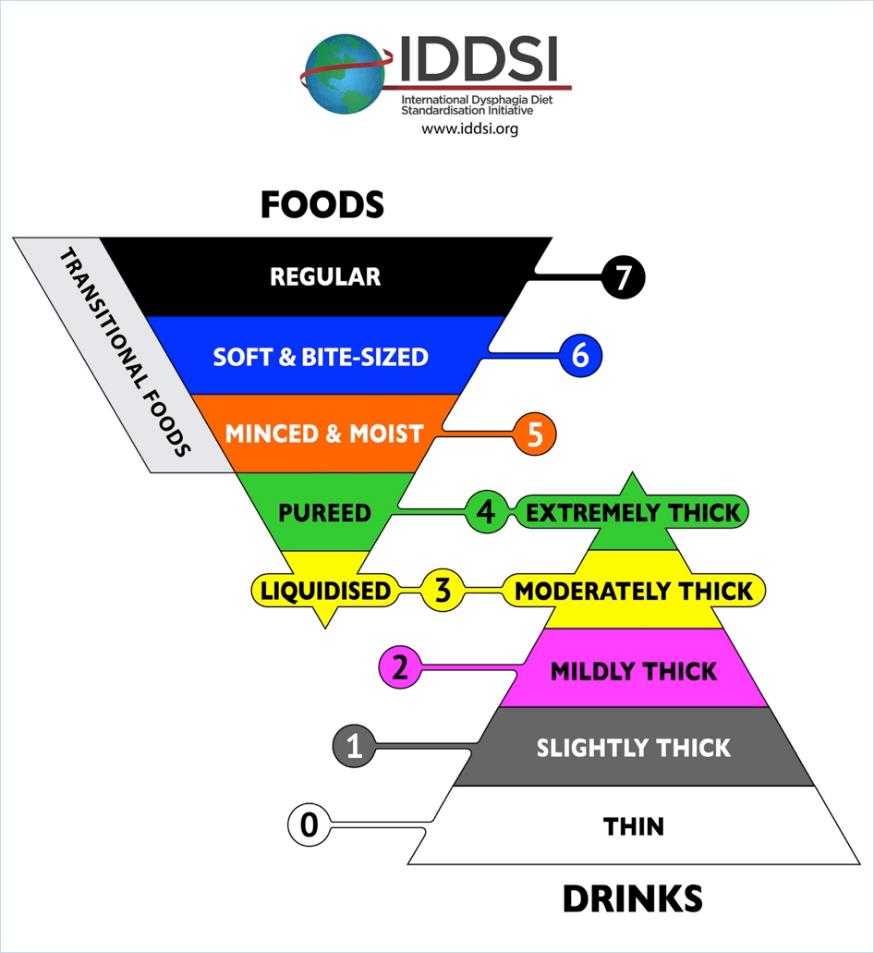
The International Dysphagia Diet Standardisation Initiative (IDDSI) is a framework to standardise terminology and offer simple testing methods to check that the preparation of the diets are correct. Dietitians New Zealand and Speech Language Therapists of New Zealand have endorsed in principle the IDDSI framework.
The goal is to reduce the risk of harm for our patients and residents due to miscommunication and poorly prepared texture modified diets. It is important to note that the framework relates to dysphagia diets only. Residents may be on a modified diet due to other factors not related to dysphagia. For example a resident with no teeth may need softer foods but can actually manage sandwiches.
The good news is that for many sites, there is very little change needed as they are already using the correct terms. The diagram above shows the new terminology and the minimal change in wording;
‘Smooth puree’ becomes pureed (which is also extremely thick fluids)
‘Minced and moist’ remains unchanged
‘Soft diet’ becomes ‘soft & bite sized’
Moderately thick and mildly thick remain unchanged for thickened fluids
The IDDSI framework assigns standard colours and numbers to assist with easily identifying texture modified foods and fluids. Some manufactures of texture modified foods and fluids are looking at ways to incorporate the terms, colours and numbers onto their food packaging.
Food and Fluid Preparation and Testing
The IDDSI framework offers simple tests to check that the thickness of the fluids or the size of the particles for modified foods are correct. The tests use forks, spoons, fingers or syringes – equipment that is readily available at sites.
With training and education on how to do these tests, kitchen staff and managers will be able to easily check their texture modified diets and thickened fluids are prepared correctly.
IDDSI App and Website
The IDDSI framework have developed many resources and videos to assist with the standardisation process.
or ask your dietitian and speech language therapist for more information.
Where to From Here?
Here are some small steps to help implement the IDDSI framework at your site:
Stop using any terms that are not on the framework. The term ‘mouli’ is not recognised and should not be used to describe a texture modified diet.
Download the app or look at the IDDSI website to familiarise yourself with the framework.
Try testing one of the textures you currently prepare. Does the ‘puree diet’ your site produce pass the spoon tilt test? Does the size of the minced food for ‘minced & moist diets’ fit between the prongs of a fork? Is the size of meat offered for residents on the ‘soft & bite size diet’ the size of your thumb nail?
Ask your dietitian or SLT for further training on the correct testing and preparation of dysphagia diets.
This article was contributed by Liz Beaglehole NZRD (Canterbury Dietitians) and Anna Miles PhD, Speech-language Therapist, Senior Lecturer, Speech Science, School of Psychology. The University of Auckland.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-07 11:57:002024-09-24 10:25:50Dysphagia Diets – Are we all understanding each other?
Our eyes see what is familiar and what they expect to see. Are we good at picking up subtle changes through your assessment processes and acting on them appropriately? The ability to see the less than obvious is essential when responsible for clinical assessment as you won’t act on those things you haven’t noticed.
On the 5th July I presented a full day seminar on a range of topics to Nurses working in aged care. During the day I made what should have been an obvious change but I have no doubt it wasn’t noticed by all. In the morning I wore a dress with a white jacket. In the afternoon I’d changed the dress for one of a different colour and pattern but retained the white jacket. I made the change during the lunch break.
When I entered the room after the lunch break three people commented straight away. I saw a small number of puzzled looks but those nurses didn’t say anything. Others didn’t seem to notice and didn’t make comment. We had three distinct groups. Those that notice and comment, those that notice but don’t comment and those that don’t notice and therefore don’t comment! Which are the nurses you’d feel safest with if it came to performing a clinical assessment on you on an ongoing basis day after day? Which differences would they notice and which wouldn’t get a second glance. Which changes would be commented on?
We need a mix of ‘detail’ thinkers and ‘big picture’ thinkers to see everything that occurs. Equally these two groups of people can complement each other. Working separately they will each only see part of what needs managing. Some over think and others don’t seem to think or reflect. Awareness of how the members of your nursing team work and think could be important in supporting you to minimise risk resulting from subtle changes occurring which may not have been addressed.
It may be beneficial to review personality types to see how your team are working separately or collectively to ensure the best outcome for residents in their care. This increased recognition of each others natural thinking styles may also enhance the ability of the team to understand each other and consciously support others differences. There are a raft of profiling tests however Myers Briggs has been around as a validated tool for a long time and may be a useful one for you and your team.
What subtle changes are occurring with your residents that you haven’t noticed? Did you see the white dress in the morning change to a black one in the afternoon? If not, what else are you not seeing that could expose someone to risk? Are any of your team seeing things but not saying anything because they don’t recognise it’s their responsibility or think someone else has commented?
When care planning, the goals or objectives developed for each aspect of care need to be measurable. This ensures you’re able to evaluate progress and determine whether the goal has been met or not. The concern is making sure an appropriate goal is set. While we look at this from a clinical perspective, we must always remember the resident as the central focus and director where they are able to provide input into what the care plan relays. People have choice within their capacity and sometimes as nurses, we may not agree with a choice made by our patients / residents in aged care.
When guiding weight management goals from a clinical perspective, Liz Beaglehole, Registered Dietitian has offered the below guide.
Ideal weight range in the care process:
Body mass index is still helpful in determining healthy weights for older adults. A healthy BMI range for adults over 65 actually shifts upwards as compared to adults. So a healthy BMI for older adults has been found to be BMI – 22 – 27kg/m2. A BMI above 32kg/m2 would suggest obesity, a BMI below 20 suggests underweight, and below 18.5 is malnourished.
To work out the BMI: (weight/height²). Example case: height = 1.5m and weight = 45kg
We need the height in metres and the weight in Kg.
The height needs to be squared. So a height of 1.5m = 2.25 when squared.
Then the BMI is the weight in Kg divided by the height²
Example: weight = 45kg divided by 2.25 = BMI of 20kg/m². This is regarded as the lower end of ideal body weight and suggests the resident is underweight for optimal health.
An ideal body weight for some who is 1.5m tall would be a BMI range of 22 – 27 so a weight range of min 50kg up to around 60kg. Basically to work out ideal body weight just enter different weights into the BMI calculation until you get to the BMI of at least 22 and then again to a BMI of around 27.
The ideal body weight may differ to the GOAL weight. The goal weight may be something that is set when the BMI is outside the ideal range but some weight changes are desirable. The goal weight is more useful and practical as it considers the weight history of the resident and the ability to achieve changes in weight. For example, a resident may be underweight with a weight of 42kg (BMI= 18.6) but they have been this weight for the past year. Ideally they would gain weight to 50kg, but this is unrealistic. The goal weight therefore becomes either weight stabilisation at 42kg or a slight weight gain to 44kg. This would still mean the resident is underweight but is realistic in what can be achieved. If the initial goal weight is achieved, a second goal weight may be identified. This may be to stabilise weight at 44kg or to gain to 45kg. etc…
This can work for overweight residents too. Using the same example height of 1.5m. Someone who weighs 78kg has a BMI of 34.6, and is obese. However, realistic weight loss to within the ideal body weight range would suggest the resident would need to lose around 18 – 28kg, which is completely unrealistic and would never be suggested for aged care. A more realistic GOAL weight would be weight stabilisation and then some weight loss. 5% weight loss can improve many health outcomes and this would be a realistic target. Weight loss of 5% is still around 4kg, which is possible but still difficult.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-07-12 17:48:002024-09-24 10:33:14Weight management goals in care planning
While most of the referrals for dietitian input in aged care facilities relates to unwanted weight loss, dietitians can be asked for input with residents who have unwanted weight gain.
What is overweight?
For many adults we use the Body Mass Index as a basis for identifying a ‘healthy weight range’. The BMI is a ration of the person’s height to their weight. (kg/m²) The BMI is not without its limitations, but generally it is a useful tool in assessing if someone is within the recommended weight range (BMI 20 – 25kg/m²), below it (underweight and malnourished) or above it (overweight and obese). For older adults, the ‘healthy weight range’ tends to shift upwards. There is evidence older adults with a BMI between 22 – 27 kg/m², have a longer life expectancy. There is evidence that older adults who have unwanted weight loss will reduce their life expectancy.
What is the aim?
The first question to ask is whether this weight gain is a cause for health concern, and if there are benefits gained from weight loss. In some cases weight gain may lead to reduced mobility, worsening blood sugar control, exacerbation of shortness of breath and gastric reflux, problems in fitting clothes, problems with ill-fitting hoists, chairs, and increased difficulty with transfers. If it agreed that weight loss would be beneficial, the first nutritional goal is to prevent further weight gain. Aim to stabilise the current weight. Weight loss may be the next goal once weight stabilisation is achieved.
How much weight to lose?
Stabilising the current weight is a good start. If weight loss is desired, set a realistic weight goal with the resident. Health benefits are noticeable with as little as 5% weight loss. A 85kg woman losing around 4kg should notice some benefits.
The goal of weight loss it to be losing body fat, not body muscle. If weight loss is too rapid, the risk is that significant muscle mass is lost. This can lead to worse health outcomes.
Involving the resident who has unwanted weight gain
A discussion with the resident about whether they are noticing any effects from the weight gain, and whether they would like to try and prevent gaining more weight, is essential. It may be useful to explain the expected health benefits possible with weight loss. Family may also like to be consulted, but the decision and the motivation really needs to come from the resident.
Just telling a resident they need to lose weight, or automatically changing their diet is not treating a resident with respect, nor providing care that is tailored to their needs. You may feel that the ‘best’ option would be to lose weight. The resident may feel different. They have the right to choose what’s right for them.
What strategies may help unwanted weight gain?
Losing weight is hard. There needs to be a reduction in the energy intake with an increase in energy output. Changes to food and changes to levels of activity are needed for optimal results. Activity and body movement are important in helping to maintain muscle mass. The diet still needs to remain nutritionally adequate, especially in terms of protein to minimise the loss of body protein too. Continue to offer quality protein foods, at main meals and tea meals.
An aged care facility menu is nutritionally balanced and tailored to ensure the nutritional needs of the residents are met. Talk with the resident about what ideas they might be happy to try to help reduce their food intake. Small changes eventually add up to significant calorie reduction. Start with changing one or two things only in the diet. If that is successful, add in other small changes.
Reducing Food Intake
Target between meal snacks such as morning tea, and/or afternoon tea. If the resident is not hungry at these times, he or she may be able to skip the food offered
Limit sweet drinks; offer water, ‘diet’ options and a sugar replacement in hot drinks
Reduce the frequency of desserts in the week, or offer lower calorie options such as fresh fruit, diet jelly, low fat yoghurt. Limit the use of cream on desserts.
Ensure the size of the main meal is a medium meal (not large), serve extra vegetables if the resident is wanting more food.
Look at the quantity of food eaten at meals. Reducing the amount slightly can help.
Target the amount eaten at ‘happy hours’ and other treat times
Try to encourage the resident to limit the amount of extra foods they may be buying and having in their room
Ask family and friends not to bring in food items. Suggest other options such as magazines, books, photo albums, flowers
Increasing activity levels
Encourage the resident to join in the home’s activities
Encourage the resident to walk more if possible, around the home, to the dining room, around the garden – short distances at first so they gain a sense of achievement
Family and friends may be able to help by joining the resident in walks or taking them on outings too
These are some ideas to try. For more information and tailored nutritional advice contact your clinical dietitian. If the resident is ready to make some changes, offer support and encouragement, to help enable their success. Be positive. As with all of us, sometimes we deviate from our own ‘diet’; we have a treat or a dessert or a second helping. Don’t judge residents, or be so strict with restricting foods. Avoid using phrases that suggest the resident is ‘being good’ or ‘being naughty’ in terms of whether they are following the agreed diet plan. There are no ‘good’ foods and ‘bad’ foods. And finally, weight loss takes time. Simply stalling the weight increase is a significant achievement. Long term encouragement and support is essential for successful and sustained weight loss.
https://agedcarecompliance.com/wp-content/uploads/2024/09/Unwanted-Weight-Gain-in-Aged-Care-Facilities.webp300300Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-06-10 12:43:002024-09-24 10:36:34Unwanted Weight Gain in Aged Care Facilities
Is a slip off a chair or off the side of the bed onto the floor a fall? Is a ‘controlled lowering’ by a staff member of a resident to the floor a fall?
When recording adverse events such as falls, it’s important for the purposes of consistent reporting and bench-marking that the same definition is used to define a ‘fall’. We suggest using the definition provided by the World Health Organisation (WHO) which states “A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level.” The WHO falls prevention guidelines also report that “Globally, falls are a major public health problem. An estimated 424 000 fatal falls occur each year, making it the second leading cause of unintentional injury death, after road traffic injuries.”
Working in aged care related services means you are interacting on a daily basis with those in the high risk category for falls. WHO also report for example, in the United States of America, 20–30% of older people who fall suffer moderate to severe injuries such as bruises, hip fractures, or head traumas. The Health Quality and Safety Commission New Zealand report “for every fall in hospital, there are five in aged residential care and another 40 at home and in the community. Between 2010 and 2012, a total of 200 people fell while in hospital care and broke their hips.“
The HCSL QA online bench-marking includes tracking of falls and falls related injuries so educating your staff to become familiar with the definition is important in ensuring data collected is accurate. Accurate data measurements also allow you to be aware of your start point for quality improvement projects which can then be measured at the end of a project to measure the degree of improvement.
In answer to the questions posed at the start of this article, if we apply the WHO definition, then both should be classified as falls. For those of you using the HCSL policy and procedure system, refer to the Falls Prevention Programme (document CS19) for more information on falls prevention.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2016-05-11 16:44:002024-09-25 02:42:14Falls – When is a fall not a fall?





{kind=link}