I am very happy to endorse your system as the information is invaluable for CNMs to analyse the data/information and make informed decisions on best practice and innovation to decrease hazards, improve outcomes, and mitigating factors for resident welfare. I’m pleased you are delving into the data to the level you are, as it’s time saving for sites in many respects, and so easy to dice and slice the information to get the trends.
CNM’s used to spend hours just writing up the collective information before the analysis, so this system is hugely time saving.
Rhonda Sherriff – Owner Chatswood Retirement Village
We are very pleased to have recently been granted 4 year MOH Certification! No corrective actions and three Continuous Improvements.
This follows on from a fully attained Partial Provisional Audit that was required prior to opening our two new wings earlier this year with no corrective actions.
Make no mistake! HCSL policies, software and support have played a major part in these accomplishments. The HCSL software we use means we have easy access to information in real time.
I started working with Gillian of HCSL shortly after I took on the role of Facility Nurse Manager at Bethsaida Retirement Village six years ago. The facility was not using Healthcare Compliance Solutions policies at the time and perhaps this was reflected in the previous audit results.
Gillian is always responsive to emails and phone calls which is critical when timely advice is required.
The HCSL regular newsletters are interesting with relevant and up to date information on issues affecting aged care.
Gillian is a lovely person to deal with. She is thoughtful, professional, pragmatic and I have always found her to be keen to help, with practical advice on any issues that might arise in the management of a retirement facility.
I thoroughly recommend HCSL to all aged care facilities.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2021-10-12 11:34:002024-09-25 12:13:26Bethsaida Retirement Village
There are lots of ‘trendy’ words in each work environment but one of the most important concepts which appears to be increasingly missing particularly in aged care nursing is that of critical thinking and reflective practice. Critical thinking is the core foundation of good nursing practice.
It is essential to evaluate what is occurring clinically for those in care and regularly reviewing what is being done for each individual resident along with what else needs to be done in order to provide the best care. The skills of critical thinking may not be instinctive for example for those nurses coming from a schooling system which promotes ‘rote’ learning and deters from challenging senior staff. To question another may be seen in some settings as disrespectful however in the field of clinical care, to challenge and question is essential. The attributes of those who critically think and reflect on nursing practice and care outcomes use evidence-based practice (EBP) guidelines including current EBP policies and procedures to form decisions.
Some of the skills of critical thinking are more important than others and certainly the ability to reflect while communicating with other members of the team is essential to safe and person centred care. The nurse who has developed critical thinking skills is able to interpret, understand and explain the meaning of information. This can be event based or data based eg; reading lab result forms. Investigating possible interventions based on the information at hand and analysing which will achieve a desired outcome is also part of reflecting and critically evaluating a clinical scenario. Assessing the value of information to determine it’s relevance, reliability and credibility in relation to a particular clinical presentation is also necessary.
There are potential barriers to optimising clinical outcomes by clinical staff when a pre-determined bias or fixed mind-set are applied to a set of data or resident clinical presentation. It’s only in the bringing together of information through evaluation, analysis, communicating, referencing EBP guidelines and a growth mind-set that care can be optimised.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2018-08-06 09:21:002024-09-24 09:22:07Critical thinking – the foundation of good nursing practice
Clinical documentation and clinical management relate to section 1.3.1 to 1.3.8 of the Health and Disability Services Standards and are referred to in section D5.4 of the ARRC. There are key reference documents which provide reference at residential care facility level which should be used in conjunction and addition to your organisation policies and procedures. These reference documents include:
Age Related Residential Care (ARRC) contract
NZS 8134:2008 Health and Disability Services Standards
Clinical best practice (EBP) guidelines – eg; Lippincott
The Code of Health & Disability Consumers Services Rights 1996
Clinical documentation errors of any type noted during audits will result in partial attainments at best. This is an indication there could be risk associated with gaps in service. In a previous article about medication management we noted that even a single signature missing off an administration signing sheet was enough for the auditor to assign a partial attainment finding.
Below are some of thecommon compliance gaps which relate to clinical documentation:
General compliancegaps
Missed signatures off notations.Not dated.Not signed by the author with a full signature.No designation written with signature.Not legible.Inconsistent structure of resident files.Unclear or unsecured archiving of documents.Privacy breaches due to clinical documents placed in a situation that allowed unauthorized viewing.
Initial assessmentsincluding InterRai
Not completed within time-frames defined in ARRC.Baseline recordings at time of admission not recorded.Assessment outcomes not used as a basis of care planning to link assessment to goals and interventions.Additional detailed assessments not reviewed in a timely manner eg; six monthly to coincide with InterRai reassessments.Failure to re-assess for each period of admission eg; respite care.
Clinical risk
Assessment not describing risk.Risk not reflected in care plan interventions.Lack of risk reviews.Level of risk noted in interRai assessments not included in care planning
Progress notes
Not recorded in on a shift by shift basis.Lack evidence of regular registered nurse input.Writing beyond the bottom line of the page.Failure to put resident identifiers on each side of each page (this applies to other clinical documents as well).Lack evidence of interventions being implemented.Lack evidence of RN response to clinical symptoms reported by care staff.Lack of evidence of rationale for PRN medication administration or the resulting effect.
Short TermCare Plans
Not developed for changes in clinical status eg; increased pain; infection; wounds, change in medication (to allow evaluation of effectiveness).24 hours plans not developed for residents displaying behaviours of concern (challenging behaviours).Not evaluated regularly (I suggested at least once every 7 days) by a Registered Nurse.Not recorded as resolved or transferred to Long Term Care Plan.Not developed to implement instructions included in General Pracitioner consultation plans recorded in notes.
Long TermCare Plan (LTCP)
Not reflective of all presenting potential and actual medical / clinical problems.Not documented within 3 weeks of the date of admission (ARRC requirement).Not changed at the time of health status / functional change.Interventions not reflective of each medical diagnosis.Interventions not changed within LTCP to reflect changes recorded in care plan evaluations.Frequency of clinical assessment for each actual clinical presentation eg; pain.Do not clearly indicate the level of function, assistance required for each component of care / support.Do not clearly evidence input and instruction from Medical or Nurse practitioner / Physiotherapist, Diversional Therapist, Dietitian,Psychiatric services for the elderly etc.
Care PlanEvaluations
Review of care plans not reflecting changes in residents health status as they occur.Not reflective of how well the care plan goals/ objectives have been met since the previous evaluation.Not completed within ARRC defined time-frames (at least six monthly).
Multi-DisciplinaryInput
Lack evidence of MDT input into care plan reviews and/or evaluations.Lack evidence of resident, Next of Kin (NOK) / Family / Whanau / EPOA input into assessment and care planning.Lack of evidence of timely referral in response to clinical presentation eg; unintentional weight loss not referred to Dietitian.Failure to evidence implementing instructions ofMedical or Nurse Practitioner eg; B/P to be recorded daily for the next 7/7 may be noted in the medical consultation notes however not evidenced as having been done.Lack evidence of notification to NOK / EPOA relating to resident adverse events, change in health status, medical consults etc.
Policy andprocedures
Not consistent with service delivery as noted in clinical documentation.
Internal audits are available through the online HCSL quality system utilised by our clients which allows tracking of compliance status and corrective actions as part of on-site quality and risk management. This means when the auditors arrive, there will be no surprises and you’ll know you’ve achieved excellence in care in conjunction with providing a compliant service.
If you have any comments to make about this article, please contact us here.
Dysphagia diets and a lack of understanding of how to implement them consistently, is increasing risk to residents in aged residential care services.
Texture modified diets are commonly used in aged care facilities to manage the risk of aspiration pneumonia and choking with eating and drinking. Residents with dysphagia may be placed on a texture modified diet following assessment with a speech and language therapist. However there are often a range of terms used for texture modified diets, and differing opinions on exactly how the diets should be prepared.
Confusion with terms, and the types of foods and fluids offered leads to increased risk of harm for the resident. This is particularly obvious when transferring from one facility to another. Information on texture modified diets is passed to the new facility who may use different terms. For example a site may report ‘this resident requires a soft diet’ and the interpretation of this diet at the new facility is to puree all food.
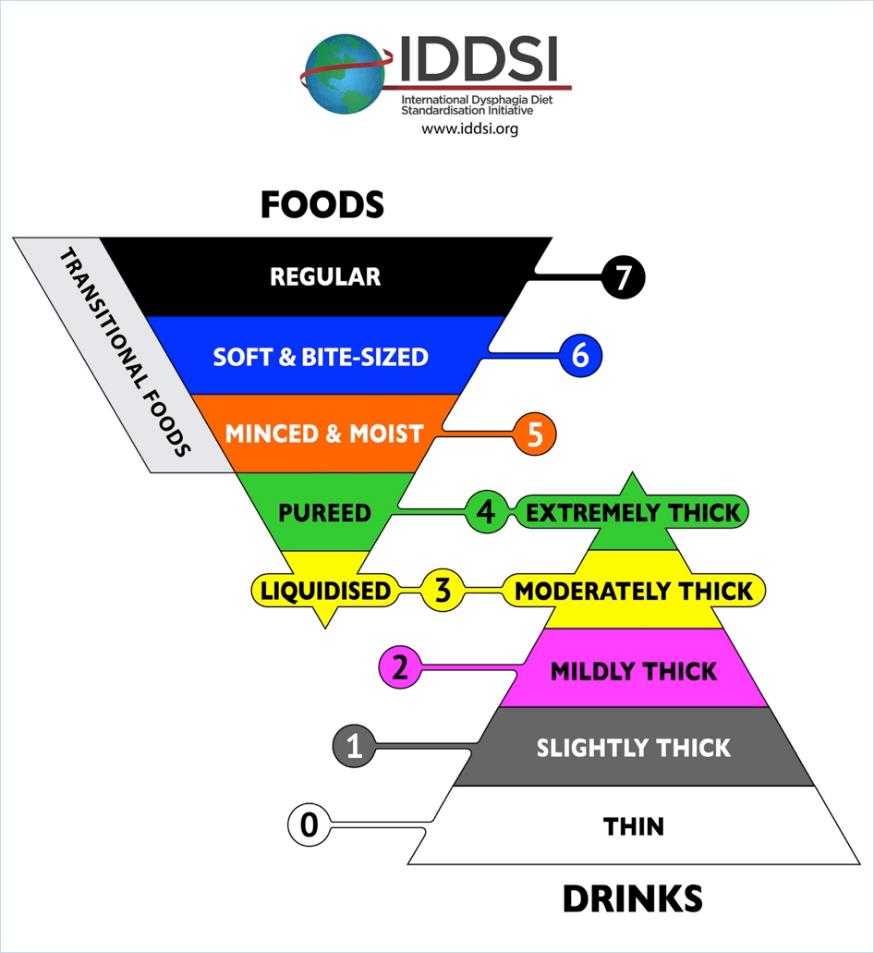
The International Dysphagia Diet Standardisation Initiative (IDDSI) is a framework to standardise terminology and offer simple testing methods to check that the preparation of the diets are correct. Dietitians New Zealand and Speech Language Therapists of New Zealand have endorsed in principle the IDDSI framework.
The goal is to reduce the risk of harm for our patients and residents due to miscommunication and poorly prepared texture modified diets. It is important to note that the framework relates to dysphagia diets only. Residents may be on a modified diet due to other factors not related to dysphagia. For example a resident with no teeth may need softer foods but can actually manage sandwiches.
The good news is that for many sites, there is very little change needed as they are already using the correct terms. The diagram above shows the new terminology and the minimal change in wording;
‘Smooth puree’ becomes pureed (which is also extremely thick fluids)
‘Minced and moist’ remains unchanged
‘Soft diet’ becomes ‘soft & bite sized’
Moderately thick and mildly thick remain unchanged for thickened fluids
The IDDSI framework assigns standard colours and numbers to assist with easily identifying texture modified foods and fluids. Some manufactures of texture modified foods and fluids are looking at ways to incorporate the terms, colours and numbers onto their food packaging.
Food and Fluid Preparation and Testing
The IDDSI framework offers simple tests to check that the thickness of the fluids or the size of the particles for modified foods are correct. The tests use forks, spoons, fingers or syringes – equipment that is readily available at sites.
With training and education on how to do these tests, kitchen staff and managers will be able to easily check their texture modified diets and thickened fluids are prepared correctly.
IDDSI App and Website
The IDDSI framework have developed many resources and videos to assist with the standardisation process.
or ask your dietitian and speech language therapist for more information.
Where to From Here?
Here are some small steps to help implement the IDDSI framework at your site:
Stop using any terms that are not on the framework. The term ‘mouli’ is not recognised and should not be used to describe a texture modified diet.
Download the app or look at the IDDSI website to familiarise yourself with the framework.
Try testing one of the textures you currently prepare. Does the ‘puree diet’ your site produce pass the spoon tilt test? Does the size of the minced food for ‘minced & moist diets’ fit between the prongs of a fork? Is the size of meat offered for residents on the ‘soft & bite size diet’ the size of your thumb nail?
Ask your dietitian or SLT for further training on the correct testing and preparation of dysphagia diets.
This article was contributed by Liz Beaglehole NZRD (Canterbury Dietitians) and Anna Miles PhD, Speech-language Therapist, Senior Lecturer, Speech Science, School of Psychology. The University of Auckland.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2017-10-07 11:57:002024-09-24 10:25:50Dysphagia Diets – Are we all understanding each other?
Our eyes see what is familiar and what they expect to see. Are we good at picking up subtle changes through your assessment processes and acting on them appropriately? The ability to see the less than obvious is essential when responsible for clinical assessment as you won’t act on those things you haven’t noticed.
On the 5th July I presented a full day seminar on a range of topics to Nurses working in aged care. During the day I made what should have been an obvious change but I have no doubt it wasn’t noticed by all. In the morning I wore a dress with a white jacket. In the afternoon I’d changed the dress for one of a different colour and pattern but retained the white jacket. I made the change during the lunch break.
When I entered the room after the lunch break three people commented straight away. I saw a small number of puzzled looks but those nurses didn’t say anything. Others didn’t seem to notice and didn’t make comment. We had three distinct groups. Those that notice and comment, those that notice but don’t comment and those that don’t notice and therefore don’t comment! Which are the nurses you’d feel safest with if it came to performing a clinical assessment on you on an ongoing basis day after day? Which differences would they notice and which wouldn’t get a second glance. Which changes would be commented on?
We need a mix of ‘detail’ thinkers and ‘big picture’ thinkers to see everything that occurs. Equally these two groups of people can complement each other. Working separately they will each only see part of what needs managing. Some over think and others don’t seem to think or reflect. Awareness of how the members of your nursing team work and think could be important in supporting you to minimise risk resulting from subtle changes occurring which may not have been addressed.
It may be beneficial to review personality types to see how your team are working separately or collectively to ensure the best outcome for residents in their care. This increased recognition of each others natural thinking styles may also enhance the ability of the team to understand each other and consciously support others differences. There are a raft of profiling tests however Myers Briggs has been around as a validated tool for a long time and may be a useful one for you and your team.
What subtle changes are occurring with your residents that you haven’t noticed? Did you see the white dress in the morning change to a black one in the afternoon? If not, what else are you not seeing that could expose someone to risk? Are any of your team seeing things but not saying anything because they don’t recognise it’s their responsibility or think someone else has commented?
Is a slip off a chair or off the side of the bed onto the floor a fall? Is a ‘controlled lowering’ by a staff member of a resident to the floor a fall?
When recording adverse events such as falls, it’s important for the purposes of consistent reporting and bench-marking that the same definition is used to define a ‘fall’. We suggest using the definition provided by the World Health Organisation (WHO) which states “A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level.” The WHO falls prevention guidelines also report that “Globally, falls are a major public health problem. An estimated 424 000 fatal falls occur each year, making it the second leading cause of unintentional injury death, after road traffic injuries.”
Working in aged care related services means you are interacting on a daily basis with those in the high risk category for falls. WHO also report for example, in the United States of America, 20–30% of older people who fall suffer moderate to severe injuries such as bruises, hip fractures, or head traumas. The Health Quality and Safety Commission New Zealand report “for every fall in hospital, there are five in aged residential care and another 40 at home and in the community. Between 2010 and 2012, a total of 200 people fell while in hospital care and broke their hips.“
The HCSL QA online bench-marking includes tracking of falls and falls related injuries so educating your staff to become familiar with the definition is important in ensuring data collected is accurate. Accurate data measurements also allow you to be aware of your start point for quality improvement projects which can then be measured at the end of a project to measure the degree of improvement.
In answer to the questions posed at the start of this article, if we apply the WHO definition, then both should be classified as falls. For those of you using the HCSL policy and procedure system, refer to the Falls Prevention Programme (document CS19) for more information on falls prevention.
https://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svg00Allionhttps://agedcarecompliance.com/wp-content/uploads/2024/08/HCSL-Color-Logo.svgAllion2016-05-11 16:44:002024-09-25 02:42:14Falls – When is a fall not a fall?






{kind=link}