Dysphagia diets and a lack of understanding of how to implement them consistently, is increasing risk to residents in aged residential care services.
Texture modified diets are commonly used in aged care facilities to manage the risk of aspiration pneumonia and choking with eating and drinking. Residents with dysphagia may be placed on a texture modified diet following assessment with a speech and language therapist. However there are often a range of terms used for texture modified diets, and differing opinions on exactly how the diets should be prepared.
Confusion with terms, and the types of foods and fluids offered leads to increased risk of harm for the resident. This is particularly obvious when transferring from one facility to another. Information on texture modified diets is passed to the new facility who may use different terms. For example a site may report ‘this resident requires a soft diet’ and the interpretation of this diet at the new facility is to puree all food.
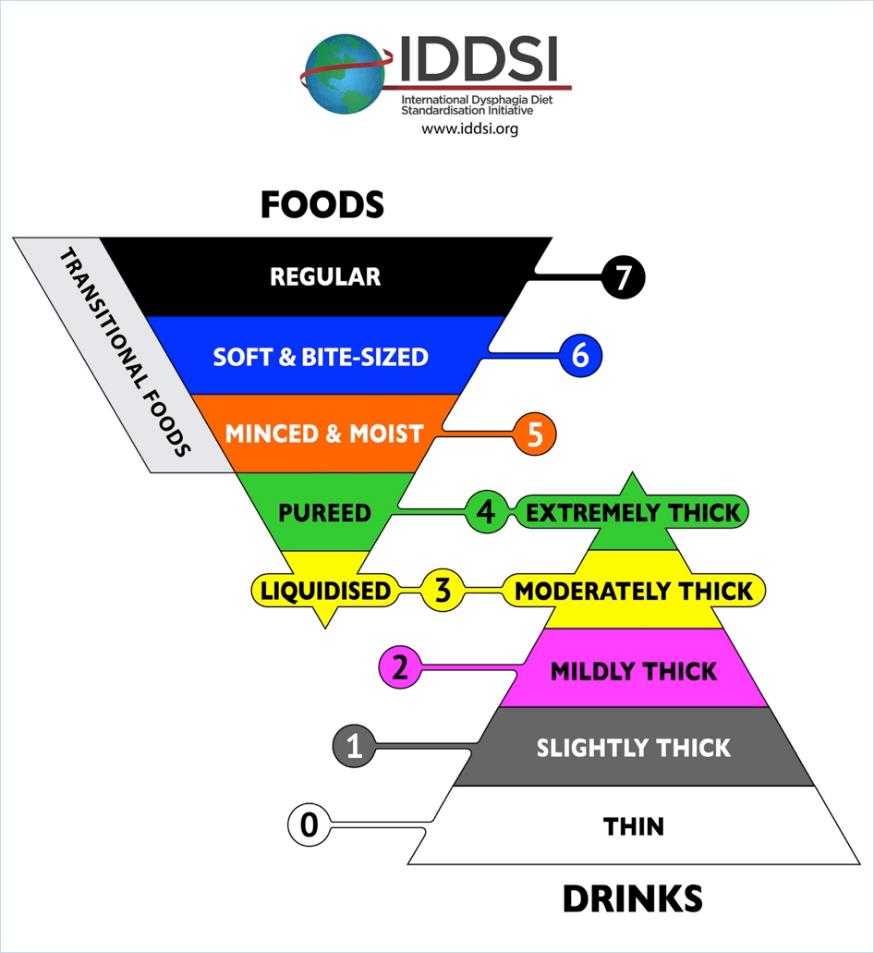
The International Dysphagia Diet Standardisation Initiative (IDDSI) is a framework to standardise terminology and offer simple testing methods to check that the preparation of the diets are correct. Dietitians New Zealand and Speech Language Therapists of New Zealand have endorsed in principle the IDDSI framework.
The goal is to reduce the risk of harm for our patients and residents due to miscommunication and poorly prepared texture modified diets. It is important to note that the framework relates to dysphagia diets only. Residents may be on a modified diet due to other factors not related to dysphagia. For example a resident with no teeth may need softer foods but can actually manage sandwiches.
The good news is that for many sites, there is very little change needed as they are already using the correct terms. The diagram above shows the new terminology and the minimal change in wording;- ‘Smooth puree’ becomes pureed (which is also extremely thick fluids)
- ‘Minced and moist’ remains unchanged
- ‘Soft diet’ becomes ‘soft & bite sized’
- Moderately thick and mildly thick remain unchanged for thickened fluids
Food and Fluid Preparation and Testing
The IDDSI framework offers simple tests to check that the thickness of the fluids or the size of the particles for modified foods are correct. The tests use forks, spoons, fingers or syringes – equipment that is readily available at sites.
With training and education on how to do these tests, kitchen staff and managers will be able to easily check their texture modified diets and thickened fluids are prepared correctly.
IDDSI App and Website
The IDDSI framework have developed many resources and videos to assist with the standardisation process.
Download the app https://play.google.com/store/apps/details?id=com.appdataroom.iddsi&hl=en
or go to www.IDDSI.org
or ask your dietitian and speech language therapist for more information.
Where to From Here?
Here are some small steps to help implement the IDDSI framework at your site:
- Stop using any terms that are not on the framework. The term ‘mouli’ is not recognised and should not be used to describe a texture modified diet.
- Download the app or look at the IDDSI website to familiarise yourself with the framework.
- Try testing one of the textures you currently prepare. Does the ‘puree diet’ your site produce pass the spoon tilt test? Does the size of the minced food for ‘minced & moist diets’ fit between the prongs of a fork? Is the size of meat offered for residents on the ‘soft & bite size diet’ the size of your thumb nail?
- Ask your dietitian or SLT for further training on the correct testing and preparation of dysphagia diets.
This article was contributed by Liz Beaglehole NZRD (Canterbury Dietitians) and Anna Miles PhD, Speech-language Therapist, Senior Lecturer, Speech Science, School of Psychology. The University of Auckland.







 ant circulating influenza strain in 2016 was Influenza A, H3N2, different from the previous year’s Influenza A, H1N1. Although covered by the vaccine, last year’s predominant strain changed slightly from what was covered in the vaccine and there were numerous reports of laboratory confirmed cases of young vaccinated adults who still acquired influenza. Despite this, vaccination still affords some protection and symptoms are less severe than without it. This is the same for the elderly whose uptake of the influenza vaccine is not so good – experts agree that there are still benefits from the elderly having an annual influenza vaccine.
ant circulating influenza strain in 2016 was Influenza A, H3N2, different from the previous year’s Influenza A, H1N1. Although covered by the vaccine, last year’s predominant strain changed slightly from what was covered in the vaccine and there were numerous reports of laboratory confirmed cases of young vaccinated adults who still acquired influenza. Despite this, vaccination still affords some protection and symptoms are less severe than without it. This is the same for the elderly whose uptake of the influenza vaccine is not so good – experts agree that there are still benefits from the elderly having an annual influenza vaccine.